Norman J. Pastorek, MD; Andres Bustillo, MD; Mark R. Murphy, MD; Daniel G. Becker, MD
The extended columellar strut–tip graft is a structural unit used in endonasal rhinoplasty that combines the attributes of the columellar strut and the tip graft. It is used to provide projection and contour to the nasal tip. Our goal with this study was to evaluate a 20-year experience with 155 patients who underwent rhinoplasty with the ex-tended columellar strut–tip graft. Of these, 110 underwent secondary rhinoplasty, and 45 under-went primary rhinoplasty. There were 6 patients in the secondary rhinoplasty group who experienced complications: in 3, the graft became visible postoperatively, and 3 patients had graft placement asymmetry. These 6 patients underwent surgery in the initial years of graft development. One patient with graft edge visibility and 1 patient with graft asymmetry underewent revision surgery with satisfactory results. The extended columella strut–tip graft is a reliable method to provide nasal tip projection and contour. The successful use of the graft requires precise diagnosis and surgical technique. Arch Facial Plast Surg. 2005;7:176-184
Author Affiliations: Departments of Otolaryngology, New York Presbyterian Hospital–Weill Medical College of Cornell University (Dr Pastorek), Division of Facial Plastic & Reconstructive Surgery, New York University School of Medicine (Dr Bustillo), New York; and University of Pennsylvania, Philadelphia (Dr Becker). Dr Murphy is in private practice in West Palm Beach, Fla.
The consistent ability to gain and maintain nasal tip projection in the underprojected nose is the trump card of the successful facial plastic surgeon. Various techniques are available to increase tip projection, so the selection is based on the surgeon’s preference and approach, the need for additional rotation, and a variety of anatomic factors. Among these are the skin– soft tissue envelope thickness and the presence of small or soft lower lateral cartilages. A careful preoperative nasal analysis and physical examination with precise anatomic diagnosis allows the surgeon to as-certain the existence of these and other factors that can play an important role in nasal tip dynamics.1
The choice of surgical technique for the control of the nasal tip is dependent on the surgeon’s armamentarium. The various techniques available include columellar struts, lateral crural steal (dome-binding) techniques, medial crural-caudal septal imbrication (tongue-in-groove techniques), medialization of the medial crural footplates, premaxillary grafting, shield-type tip grafts, and a variety of tip onlay grafts.2-8
Herein we describe a valuable technique for increasing tip projection. The ex-tended columella strut–tip graft is a powerful graft that the senior author (N.J.P.) has used for 15 years and found advantageous in specific anatomic situations.
METHODS
BACKGROUND
The extended columellar strut–tip graft is highly versatile in that it offers unique advantages in both primary and secondary rhinoplasty procedures. This graft combines the contouring shape of the tip graft with the strength of the columellar strut into a single stable unit. The extended columellar strut–tip graft is a unit construction element. It is not dependent on suturing or other tip architecture for its projection force. The graft can be used to provide a variable amount of projection and rotation. This is dependent on its placement and length. The graft can also be used just to provide contour and shape to the tip when the tip is adequately projected but asymmetric as a result of previously resected domal areas.
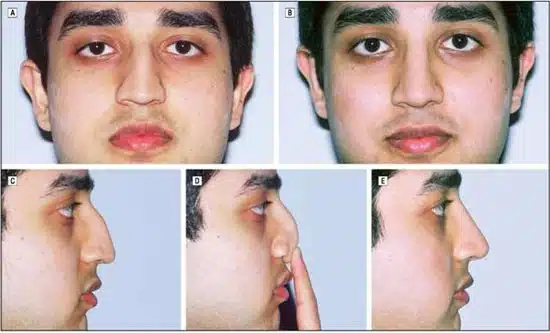
Figure 1. Preoperative (A, C, and D) and 1-year postoperative (B and E) views of a 24-year-old man who underwent primary rhinoplasty. He presented with an underprojected and amorphous nasal tip with extremely weak support. An extended columellar strut–tip graft was placed to project and define the tip.
As much information as possible should be sought about the condition of the lower lateral cartilages and previous surgical procedures. Bimanual palpation of the nasal tip under magnified illumination can reveal important information regarding the condition of the lower lateral cartilages.
In primary rhinoplasty, we consider using this graft in cases where the lower lateral cartilages ineffectively support the nasal tip, the lower lateral cartilages are small and/or soft, the high point of the dorsum is at the supratip, soft lower lateral cartilages and nasal tip ptosis are both present, and/or the nasal tip skin is very thick. Small and soft lower lateral cartilages are the cardinal anatomic feature of the underprojected tip (Figure 1 and Figure 2). In these patients, the addition of a columellar strut to the dome-binding suture may not achieve the desired projection.1 Therefore, the need for this graft in a primary rhinoplasty may not be recognized until the concluding stages of the procedure. The senior author’s use of this graft in primary rhinoplasty has increased in recent years.
The extended columellar strut–tip graft is useful in any secondary rhinoplasty when either maximum projection of the tip or tip contouring is required. In cases of secondary rhinoplasty where the cartilages are soft, this graft provides support independent of the nonsupporting soft lower lateral cartilages. The graft is also useful in cases of secondary rhinoplasty where the nasal tip skin is so thick that it resists the contouring changes of conventional endonasal tip grafts. In cases of secondary rhinoplasty where the domal region has been aggressively resected, the extended columellar strut–tip graft can provide both contour and projection independent of the lower lateral cartilages. In cases of secondary rhinoplasty where tip grafting has been done but subsequent scar tissue has overwhelmed an adequate early postoperative appearance, the ex-tended columellar strut–tip graft is beneficial (Figure 3 and Figure 4).
It should be made clear to the patient that the stiffness and resistance to pressure at the nasal tip postoperatively are inherent to the graft. If the previous rhinoplasty was done using an external approach, the columellar scar (even though not re-opened) may become and remain erythematous for a few weeks after placement of the graft. The use of this graft in a patient with thin skin requires careful shaping and placement of the graft (Figure 5).3,4
TECHNIQUE
The senior author uses an endonasal rhinoplasty approach exclusively. The lower lateral cartilages are delivered into the nares via intercartilaginous and marginal incisions. Dome-binding sutures are placed with a single 4-0 polypropylene mattress suture. The knot is placed between the domes. This provides a stable scaffold for the graft. In secondary rhinoplasty, the dome remnants are delivered. This dissection can be tortuous owing to scarring. The remnants, no matter how small, are sutured to provide posterior support to the graft.
Preparation of the graft requires conventional rhinoplasty instruments. A section of cartilage is obtained to fashion the graft and a columellar strut (if needed). The septum should be available for a graft measuring 2.5 to 3.0X 1.0 cm. The alter-native to septal cartilage is a section of cavum or cymba concha that can provide approximately this same amount of firm cartilage. The absence of adequate firm septal or conchal cartilage to form a single continuous entity from nasal tip to the premaxilla precludes the use of this graft. Other grafts that may be needed for the rhinoplasty must also be considered in pre-surgical planning.
All other steps required for rhinoplasty are then performed. A decision is made as to the necessity of a columellar strut in addition to the graft. The graft provides great support without the use of a strut. The independent columellar strut is used when the feet of the medial crura are very weak or short or the available cartilage material is not particularly strong. However, it is rare that a strut is needed in addition to the extended columellar strut–tip graft.

Figure 2. Preoperative (A and C) and 2-year postoperative (B and D) views of a 22-year-old woman who underwent primary rhinoplasty. She presented with an underprojected and broad nasal tip. An extended columellar strut–tip graft was used to project and define her nasal tip. Note the improvement in the double break and columellar show provided by the graft.

Figure 3. Preoperative (A and C) and 2-year postoperative (B and D) views of a 41-year-old woman who presented with a history of a rhinoplasty by another surgeon. She had a severe ptosis of the nasal tip and extremely thin skin. We used the extended columellar strut–tip graft to project and rotate the nasal tip.

Figure 4. Preoperative (A and C) and 1-year postoperative (B and D) views of a 32-year-old woman who presented with a history of 2 rhinoplasties by different surgeons. The first was carried out through an endonasal approach and the second via an external approach. We performed a tertiary rhinoplasty via an endonasal approach and used an extended columellar strut–tip graft to achieve tip projection and definition.

Figure 5. Preoperative (A and C) and 2-year postoperative (B and D) views of a 41-year-old woman who presented with a history of a rhinoplasty by another surgeon. She presented with a weak nasal tip, a nasal high point at the anterior septal angle, and extremely thin skin. An extended columellar strut–tip graft was placed to achieve adequate nasal tip projection.
If an independent strut is needed, it is positioned after the placement of the dome-binding and septal-columellar su tures. The strut extends from just below the domes to just above the premaxilla. It is placed into a pocket dissected with a curved Stevens scissors at a separate mid-columellar marginal incision. The strut is spring loaded in the intercrural space to provide medial support. The incision is then closed with 1 suture (4-0 chromic).
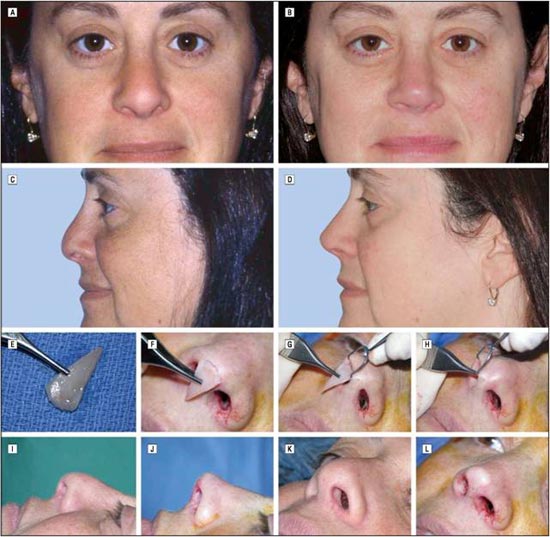
Figure 6. Preoperative (A and C), 6-month postoperative (B and D), and intraoperative (E-L) views in the case of a 45-year-old woman who presented with a history of a rhinoplasty by another surgeon. Note the preoperative underprojected tip and poor support (A and C) secondary to an aggressive resection of the lower lateral cartilages. The extended columellar strut–tip graft (E) was placed via a right marginal incision (F-H). Also shown intraoperatively are lateral views before (I) and after (J) graft placement and oblique views before (K) and after (L) graft placement.
The placement of the extended columellar strut–tip graft is the final maneuver of the rhinoplasty. All incisions except the right marginal one are closed with interrupted chromic sutures. An approximate length measurement is made between the base of the columella and the new desired tip position. We make the graft somewhat larger than this measurement be-cause, if need be, it can always be made shorter but not longer (Figure 6 and Figure 7).
The basic shape of the graft is a long isosceles triangle with the 2 long sides slightly curved inward. The shape of the long sides and the width of the triangle are determined by the shape and length of the columella. The flaring toward the base of the triangle is determined by the width of the infratip lobule and the tip of the nose. The appearance of the final graft is similar to the silhouette of agolf tee with a rounded rather than a flat top. The base should be round and thinned so that it is extremely flexible and nearly transparent at the most peripheral millimeter. In patients with thin skin, this is essential to avoid graft visibility. The final length of the graft will depend on the objective of the operation. Grafts range in length from 2 to 3 cm. The width varies from 8 to 10 mm for women and 10 to 12 mm in men. When used for tip contouring, the graft will need to be trimmed at the apex so that it does not augment projection. Grafts used for projection will have a longer span. Herein lies the versatility of the graft.
Once the graft has been prepared, the marginal incision on the right side is extended slightly onto the columella, if necessary, to accommodate the graft. A pocket is then made very carefully in the precrural columellar space with the curved Stevens scissors. The region over the domes and supratip area should be widely undermined.
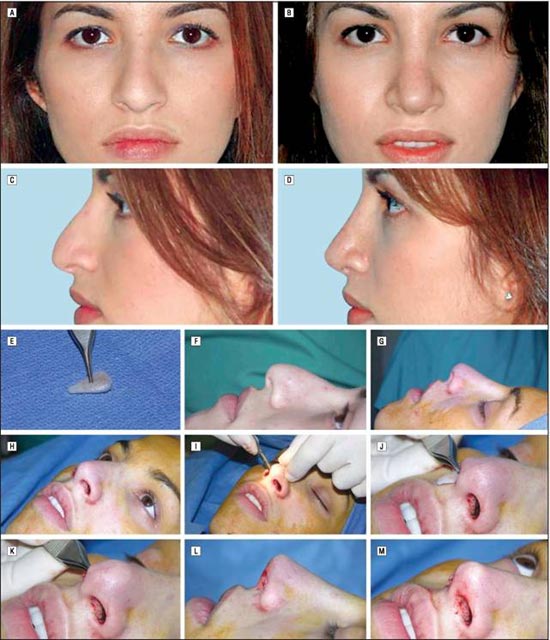
Figure 7. Preoperative (A and C), 2-month postoperative (B and D), and intraoperative (E-M) views in the case of a 22-year-old woman who underwent primary rhinoplasty. She presented with a broad, underprojected, and ptotic nasal tip (A and C). The extended columellar strut–tip graft was used to project and define the tip. The supratip area still demonstrates postoperative edema (B and D) that will resolve. Panel E shows the size and shape of the graft; F, the operative view just before the procedure was begun. Panels G and H show the lateral and oblique views, respectively, after placement of the dome-binding sutures. Although this provided some projection, additional projection and strength were needed for an optimal result in this patient. Panels I, J, and K show the placement of the graft through the right marginal incision. Panels L and M show the lateral and oblique views, respectively, after placement of the graft.
The graft is grasped at its center with Brown-Adsen forceps and slipped through the right marginal incision with the base directed toward the nasion and the sharp-angled apex directed toward the nasal tip. In this manner, the graft is placed over the nasal dorsum. The graft is then moved slowly downward toward its final position with the Brown-Adson forceps, directing the narrow portion of the graft into the precrural columellar space until it is firmly seated just above the premaxilla. The graft should not be forced. If the pocket is not large enough, as determined by resistance, the graft is withdrawn and the pocket enlarged or the long portion of the graft reduced in width. The graft is firmly placed with the use of both thumbs and index fingers until it is seated in position. The graft will maintain position because of the long slender pocket made in the precrural space. The purpose of the graft determines its position relative to the domal area. Grafts used for projection are placed with the base riding above the domes. When used for contour, the base is placed at the level of the domes (Figure 8 and Figure 9)

Figure 8. Preoperative (A and C) and 2-year postoperative (B and D) views of a 45-year-old woman who presented with a history of a rhinoplasty by another surgeon. Her lower lateral cartilages had been aggressively resected, and the nasal high point was at the anterior septal angle. The extended columellar strut–tip graft was used to provide definition and support to the nasal tip.
The only incision remaining open is the marginal incision on the right side. This incision is now closed with 1 or 2 sutures (4-0 chromic). It is important that 1 of the sutures be placed in the mucosa at the apex of the nostril to provide stability to the graft. A small Telfa wick (Tyco Healthcare, King of Prussia, Pa) is placed into each nare, and a splint is placed over the nasal dorsum.
Postoperative follow-up includes the routine removal of bandages on the sixth or seventh postoperative day. At 1 month, a decision is made whether to inject 0.01 mL of triamcinolone (10 mg/mL) into the supratip subcutaneous space. The decision is based on the presence of accumulated immature scar tissue obliterating the supratip break. The need for triamcinolone injection is more common in thick-skinned patients than in patients with thin skin.
When used for an underprojected tip, the graft can provide significant projection. The projection at the time of surgery is approximately 2 mm greater than the final projection will be 6 months postoperatively. The graft provides an elegant unit nasal tip with a double break.
RESULTS
The extended columellar strut–tip graft was used in 155 rhinoplasties, 110 secondary rhinoplasties, and 45 primary rhinoplasties. There were 6 complications, all occurring in the secondary rhinoplasty group and all during the first years that the graft was used. The problems were graft edge visibility in 3 patients and graft placement asymmetry in 3 patients. One patient underwent revision surgery for correction of the edge visibility with a satisfactory outcome, and 1 patient had the tip graft satisfactorily repositioned. In the other cases of slight graft asymmetry or edge visibility, the patients found increased projection alone to be acceptable, after years of living with a wide polly beak tip–type tip. These patients elected to not undergo further adjustment of the graft (Figure 10).
COMMENT
The extended columellar strut–tip graft was evolved from the Sheen tip graft.5 The senior author first used the Sheen graft in the early 1980s in an attempt to bring projection and form into secondary rhinoplasty cases when the lower lateral cartilages, following surgery, were ineffective in maintaining support. The nasal tips in these patients displayed a wide variety of problems: some had very thick skin; others had separation and retraction of the domes; and in some, the lower lateral cartilage remnants were barely palpable. All tips had the rounded, blunted, formless appearance characteristic of lower lateral cartilage excision in noses with underprojection before primary surgery.
Sheen tip grafts were placed in a pocket dissected in the infralobular area to accept the triangular (shield) cartilage graft. The pocket was made the same size as the graft. While the immediate appearance was pleasing, the long-term appearance was decidedly not pleasing. In each of the cases, circumferential scarring occurred, contracting the tissue at the graft edge. This brought the graft edge into severe relief. One patient descibed the appearance as that of a dime in the tip of the nose. It became apparent that an exact pocket, while it might work elsewhere in the nose, was not appropriate at the nasal tip, perhaps because the tip is curved in both a horizontal and a vertical direction. The graft concept was good, but an-other approach had to be developed to make it work in our setting.
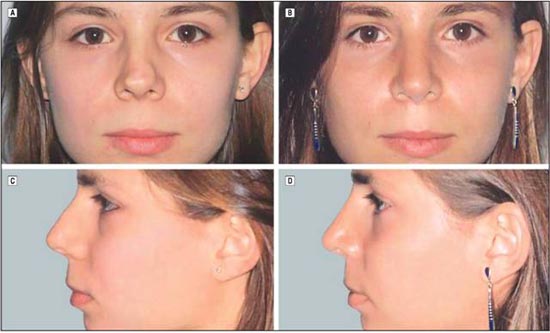
Figure 9. Preoperative (A and C) and 18-month postoperative (B and D) views of a 21-year-old woman who presented with a history of a rhinoplasty by another surgeon. She demonstrated nasal tip bossae as well as a deficiency of the right upper lateral cartilage. An extended columellar strut–tip graft was used to define the nasal tip without adding projection.

Figure 10. This figure demonstrates one of the first extended columellar strut–tip grafts placed by the senior author (N.J.P.) nearly 15 years ago: preoperative (A) and 2-year postoperative (B) views of a 40-year-old woman who presented with a history of a rhinoplasty by another surgeon. She underwent placement of the graft for improvement in nasal tip projection and definition. In panel B, the graft is clearly visible on the right side of the tip. A wide undermining of the tip and supratip along with a precise carving of the graft is necessary to prevent this complication.
The next step was a larger graft placed in the tip after wide rhinoplasty soft tissue envelope undermining. The graft was secured in the middle to distal columella with a temporary 4-0 polypropylene suture. This wide under-mining eliminated the scar contracture problem. Al-though these anchored tip grafts gave shape and form to the nasal tip, the use of a strut was required when a major projection deficit existed. The extended columellar strut–tip graft was a natural progression in the quest to provide both form and support to the major underprojected tip.
The use of this graft has enhanced the control of the nasal tip. It was first developed to provide projection in secondary cases but has evolved in recent years to in-creasing use in primary rhinoplasty. Its reliability and safety have been established.
A multitude of other grafting techniques are also avail-able to increase tip projection. Porter et al6 have de-scribed a contoured auricular projection graft as an alternative onlay graft to achieve increased projection in endonasal rhinoplasty. They found this technique particularly useful for rhinoplasties in Asian and African American patients and in certain revision rhinoplasties. Projection is achieved without rotation. Via an endonasal approach, a precise pocket is prepared, and the graft is placed above the domes to achieve the desired projection. This graft can also be secured into place when the surgeon undertakes an external rhinoplasty approach. Porter et al believe that this approach yields a more rounded nasal tip than other tip grafts and results in a more natural-appearing tip in specific rhinoplasty populations.
The external rhinoplasty approach allows sutured-inplace shield-shaped tip grafts to increase tip projection and improve tip contour to camouflage aysmmetries.2-4 The graft is sutured to the caudal margins of the medial/ intermediate crura that have been stabilized by the sutured-in-place columellar strut. Some surgeons recommend cutting the graft larger at the leading edge to allow in situ carving once the graft is secured into position.2
The extended columellar strut–tip graft is a very versatile graft for the endonasal rhinoplasty surgeon. The graft achieves a refined nasal tip. It is useful in any primary or secondary rhinoplasty where maximum projection of the tip is required. It is extremely valuable for secondary rhinoplasty in which tip contouring is needed for tip asymmetries or resected domes. It has been used by one of us (N.J.P.) for more than 15 years and is a useful addition to the armamentarium of the rhinoplasty sur-geon. The extended columellar strut–tip graft is a unit construction element; it is not dependent on suturing to other tip architecture for its projection force. The graft is not sutured. Its placement is secured by the development of a tight pocket in the precrural space and the tension-exerting forces of the graft. The senior author has not encountered problems with graft shifting over time. Immediate slight shifting to the right was noted in 3 of the cases with complications during the first 18 months the graft was used. Once tight suture closure of the right marginal incision and superior columellar incision was recognized as a very significant stabilizing maneuver, the shifting problem was controlled.
The key technical points of the extended columella strut–tip graft merit review. The longest possible cartilage graft is obtained from the septum or from the cavum or cymba concha. The dimensions of the graft are typically 2.5 cm in length by 8 to 12 mm in width at the leading edge (base). Surgeons tend to make tip grafts too narrow. For men, the tip grafts should generally be wider and typically measure 10 to 12 mm in width at the leading edge. The leading edge in women should be 8 to 10 mm. The base is thinned at its periphery making it flexible against the tip skin. The thinned cartilage will curve to give softness at the leading edge rather than a distinct visible cartilage edge. Excessively stiff tip grafts should be crosshatched on the caudal surface to allow cephalic bending. The flexibility provides an elegant double break. All edges of the tip graft should be rounded off to pre-vent visibility of the edges.
If the medial crura are extremely weak and nonsupportive, a strut should be placed. The dome remnants are bound with a 4-0 polypropylene mattress suture. In preparation for the graft, all mucosal incisions except for the right marginal incision are closed with 4-0 chromic sutures. A pocket is made in the precrural space down to the premaxilla. The graft is placed first onto the nasal dorsum and then is slowly moved into the precrural space. The graft is then manipulated into place using both thumbs and index fingers. The right marginal incision is then closed with 4-0 chromic sutures.
Accepted for Publication: February 15, 2005. Correspondence: Andres Bustillo, MD, 18 E 88th St, New York, NY 10128 (andresbustillo@yahoo.com).
REFERENCES
- Pastorek N, Ham J. The underprojecting nasal tip: an endonasal approach. Facial Plast Surg Clin North Am. 2004;12:93-106.
- Toriumi DM, Becker DG. Rhinoplasty Dissection Manual. Philadelphia, Pa: Lippincott Williams & Wilkins; 1999.
- Johnson CM, Toriumi DM. Open Structure Rhinoplasty. Philadelphia, Pa: WB Saunders; 1990.
- Toriumi DM, Johnson CM. Open structure rhinoplasty: featured technical points and long-term follow-up. Facial Plast Surg Clin North Am. 1993;1:1-22.
- Sheen JH, Sheen A. Aesthetic Rhinoplasty. 2nd ed. St Louis, Mo: CV Mosby Co;
1987. - Porter JP, Tardy ME, Cheng J. The contoured auricular projection graft for nasal tip projection. Arch Facial Plast Surg. 1999;1:312-315.
- Kridel RW, Scott BA, Foda HM. The tongue-in-groove technique in septorhinoplasty: a 10-year experience. Arch Facial Plast Surg. 1999;1:246-256.
- Kamer FM, Churukian MM. Shield graft for the nasal tip. Arch Otolaryngol. 1984; 110:608-610.